

Background
Diffuse large B-cell lymphoma (DLBCL) is the most common aggressive non-Hodgkin lymphoma subtype with a 5-year survival of ~64%. While DLBCL is treated using immunochemotherapy (IC) with curative intent, 20%-40% of patients do not reach remission or relapse post IC. Clonal somatic mutations have been associated with aging, hematologic malignancies (predominately myeloid), and reduced OS in the general population. The objective of this study was to evaluate the association of clonal somatic mutations with event-free survival (EFS) and overall survival (OS).
Methods
We studied newly diagnosed DLBCL cases treated with IC who were enrolled in the Molecular Epidemiology Resource (MER) of the University of Iowa/Mayo Clinic Lymphoma Specialized Program of Research Excellence (SPORE). Clinical and treatment data were abstracted from medical records and all patients were systematically followed for disease outcomes. Pre-treatment DNA was extracted from matched peripheral blood and paraffin-embedded tumor tissue, and whole exome sequencing was conducted at 100x coverage. From the peripheral blood, allele counts from GVCF files produced by HaplotypeCaller in GATK were extracted for 42 genes commonly associated with clonal hematopoiesis (e.g. DNMT3A, TET2, and ASXL1). Mutations were deemed clonal somatic if the population minor allele frequency was <0.5% in ExAC and had a variant allele fraction (VAF) that deviated from 0.5 using a binomial distribution test at p<0.001. Furthermore, mutations had to have a minimum alternate read count of at least 5 reads, a VAF greater than or equal to 10%, and met at least one of the following criteria: CAVA impact of "HIGH"; pathogenic/likely pathogenic per ClinVar; or reported in COSMIC at least 10 times. EFS was defined as time from diagnosis to disease progression, relapse, retreatment, or death due to any cause. The association of clonal somatic mutations with prognosis was estimated using Kaplan-Meier curves, and hazard ratios (HR) and 95% confidence intervals (CI) from Cox regression. Associations were adjusted for age at diagnosis, sex, and the International Prognostic Index (IPI).
Results
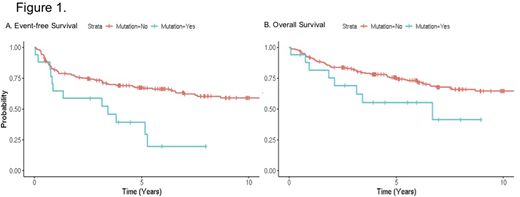
The study consisted of 261 DLBCL patients treated with IC. The median age at diagnosis was 65 years (range 20-90) and 56% were male. With a median follow-up time of 5.1 years (range 0.1-15.0), there were 100 events and 80 deaths. A total of 17 (6.5%) patients had clonal somatic mutations, and16 patients were over the age of 60. A total of 8 (of 42) genes had clonal somatic mutations, with SF3B1, ASXL1, and TET2, being the most frequent (4 individuals per gene). VAFs ranged from 0.10 to 0.28 and none of the patients had multiple mutations. Additionally, the clonal somatic variants found in the peripheral blood were abscent in the tumor sample. Of the 17 patients with clonal somatic mutations, 12 had an event while 88 patients without a mutation had an event. In a univariate analysis, clonal somatic mutations were associated with inferior EFS (HR=2.55, 95% CI 1.39-4.68, p=0.002; Figure 1A). After adjusting for age, sex, and IPI, clonal somatic mutations remained associated with inferior EFS (HR=2.02, 95% CI 1.09-3.74, p=0.026). Clonal somatic mutations were also associated with inferior OS in the univariate analysis (HR=2.06, 95% CI 0.99-4.29, p=0.053), which attenuated after multivariate adjustment (HR=1.59, 95% CI: 0.76-3.34, p=0.22, Figure 1B). Although based on small numbers, mutations in SF3B1 were associated with inferior EFS (HR=3.25, 95% CI 1.16-9.12, p=0.025), but did not reach significance for OS (HR=2.56, 95% CI 0.78-8.38, p=0.120).
Conclusions
In this novel study of newly diagnosed DLBCL patients, clonal somatic mutations were identified in 6.5% of patients and were associated with inferior outcomes. Additional research is required at deeper sequencing to validate these findings and integration with tumor genomics is required to understand the prognosis of DLBCL patients with smaller clonal populations.
Shah:Dren Bio: Consultancy. Maurer:Celgene / BMS: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees; Morphosys: Membership on an entity's Board of Directors or advisory committees; Kite: Membership on an entity's Board of Directors or advisory committees; Nanostring: Research Funding. Martin:Celgene: Consultancy; Karyopharm: Consultancy, Research Funding; Morphosys: Consultancy; Regeneron: Consultancy; Incyte: Consultancy; Kite: Consultancy; Cellectar: Consultancy; Bayer: Consultancy; Beigene: Consultancy; Sandoz: Consultancy; I-MAB: Consultancy; Janssen: Consultancy; Teneobio: Consultancy. Witzig:AbbVie: Consultancy; Incyte: Consultancy; Acerta: Research Funding; Karyopharm Therapeutics: Research Funding; Immune Design: Research Funding; Spectrum: Consultancy; Celgene: Consultancy, Research Funding; MorphSys: Consultancy. Nowakowski:NanoString: Research Funding; Seattle Genetics: Consultancy; Curis: Consultancy; Kymera: Consultancy; Kite: Consultancy; Ryvu: Consultancy, Membership on an entity's Board of Directors or advisory committees; MorphoSys: Consultancy, Research Funding; Celgene/BMS: Consultancy, Research Funding. Novak:Celgene/BMS: Research Funding. Cerhan:NanoString: Research Funding; BMS/Celgene: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal